Nursing Diagnoses
1. Ineffective Childbearing Process R/T Substance Abuse AEB lack of prenatal visits, mother does not report appropriate pre and postpartum lifestyle because of substance abuse, has limited support systems
This nursing diagnosis describes the mothers impaired ability to safely manage her pregnancy. This relates to her failure to obtain prenatal care before birth, her lifestyle of drug use that cannot safely support an infant, and the possibility that she is not well supported by friends, family or significant others.
2. Risk for disturbed Maternal/Fetal Dyad R/T substance abuse AEB challenging feedings, mother unable to adequately care for her infant, involvement of social services
This nursing diagnosis describes the possible problems between the mother and infant that may occur after birth. Their relationship may be disrupted by the symptoms of NAS the infant will experience which can be very traumatic for both the baby and the mother. It also involves the mothers inability to provide the care the infant needs. Finally, the required involvement of social services may lead to removal of the infant from the mother's care. This can be traumatic for both the infant and the mother. Watch the video below to see an expectant mother's experience with NAS and her desire to get help for her next infant.
This nursing diagnosis addresses the potential problems infants affected by NAS may have in breastfeeding. Often, the symptoms of NAS involve excessive crying, irritability and inability to self-calm which infants should normally be able to do in order to begin breastfeeding. Mothers of infants with NAS often have many challenges breastfeeding. Healthcare professionals must be available to help the mother and assist her with breastfeeding.
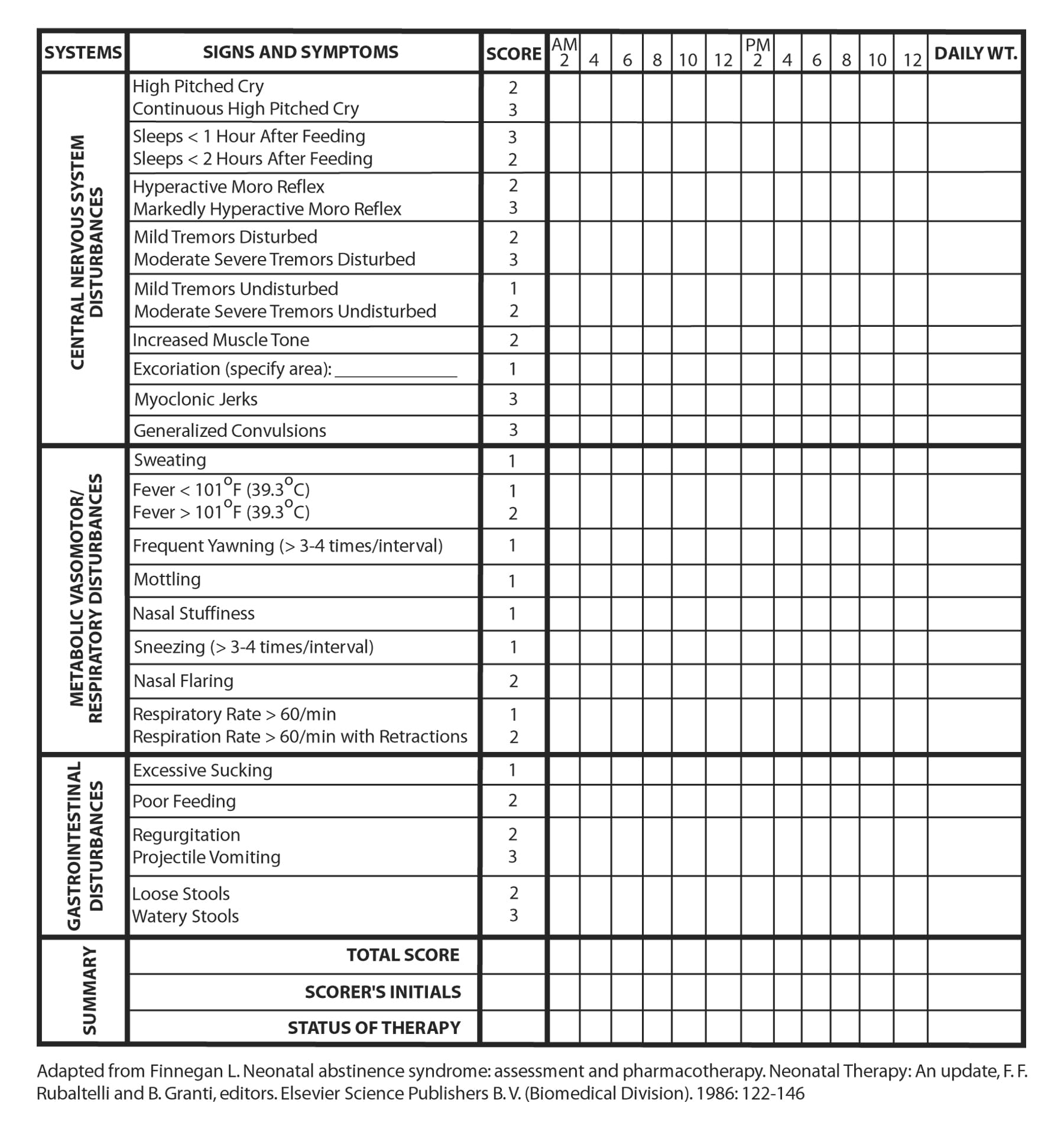
4. Disorganized infant behavior R/T prenatal substance abuse AEB tremors, jitteriness, hyperactivity, fever, sweating, nasal flaring, respiratory distress, poor feeding, myoclonic jerking, seizures, GI disturbances
This diagnosis describes the challenges the infant may have in adjusting to new life with the onset of traumatic withdrawal syndromes. The symptoms listed above could develop into dangerous conditions such as serious breathing complications, inability to self-regulate temperature, malnutrition, brain damage and extreme fatigue. For more information about symptoms of NAS click here for a link to an earlier blog post.
This diagnosis describes the challenges the infant may have in adjusting to new life with the onset of traumatic withdrawal syndromes. The symptoms listed above could develop into dangerous conditions such as serious breathing complications, inability to self-regulate temperature, malnutrition, brain damage and extreme fatigue. For more information about symptoms of NAS click here for a link to an earlier blog post.

The challenges faced by the drug-addicted mother and her
infant suffering from NAS are extensive and have emotional, physiological and
social implications as explained above. Expectant mothers who are addicted to
substances must seek support from their local birthing center, primary care
provider, addiction support facilities, and other community resources to ensure
safe pregnancy and delivery, and to ensure their newborn starts life with the
highest quality care and attention.



















{kind=link}