Research has discovered some treatment interventions that should be done, and some that shouldn't. For example, Naloxone, the medication used to reverse dangerous side effects of opiate overdose such as respiratory depression, is contraindicated for NAS-affected infants. It has been shown to exacerbated the symptoms of NAS and can bring on seizures in withdrawing infants (Kocherlakota, 2014).
Non-Pharmacologic Treatment
 |
| Figure 1. Swaddling |
- Reducing environmental stimuli (dimming lights, turning down loud sounds)
- Avoiding self-stimulation (swaddling, careful/comfortable positioning, swaying, rocking)
- Responding to infant's physiologic needs (providing high-calorie formula or breast milk to stimulate growth)
(Hudak, Tan, The Committee on Drugs, & The Committee on Fetus and Newborn, 2012).
Pharmacological Treatment
The most effective pharmacological treatment regimen that has been researched is a weaning system involving either morphine or methadone. In the table below, these two front line medications are compared.
Treatment
|
Dosage
|
Action
|
Notes
|
Cons
|
Morphine
|
0.05 mg/kg per day to 1.3 mg/kg per day
|
Decreases incidence of seizures, improves feeding, decreases
irritability.
|
Most commonly used method of pharmacological treatment, solution is
stable and easy to administer via oral route, the dosage is also easily
titrated because of the short half-life of morphine
|
Increases length of hospital stay, must be administered every 3-4
hours because of the short half-life of morphine
|
Methadone
|
Similar to that of morphine
|
Well absorbed via oral route of administration, has a long half life which decreases the number of needed administrations
|
Difficult to titrate because of the long half-life of methadone
|
|
(Hudak, Tan, The Committee on Drugs, &
The Committee on Fetus and Newborn, 2012), (Kocherlakota, 2014)
|
||||
Treatment plans are heavily influenced by scores collected via the Neonatal Abstinence Syndrome Scoring System (click here). Based on a treatment plan like the one in Figure 2, using a standardized scoring system, a score of ≥8 three time in a row, or 1 score of ≥12 triggers medication administration. At each reassessment of the neonate, medication dosing may increase or decrease based on the withdrawal symptoms shown by the infant.
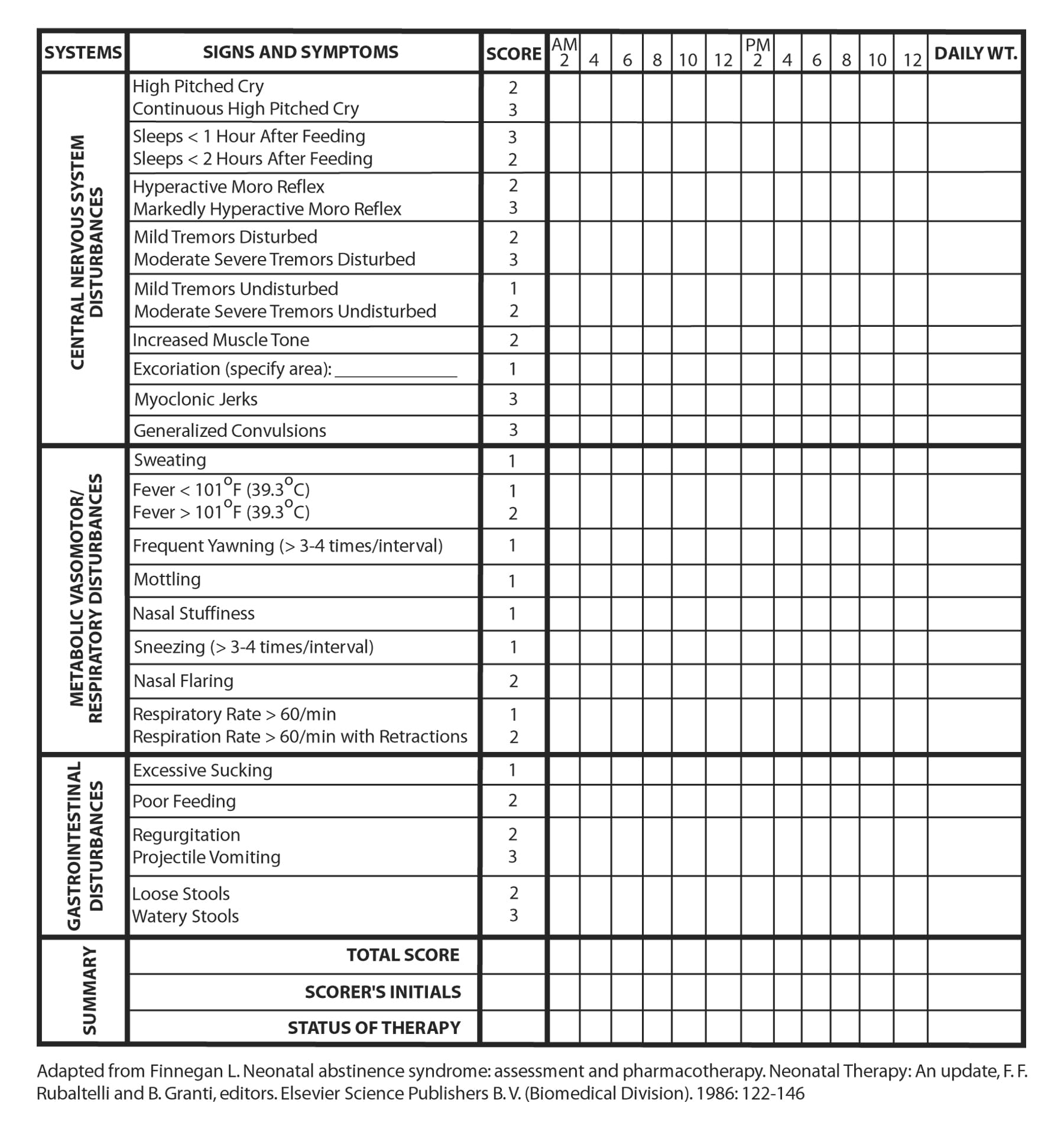{kind=link}
 |
| Figure 2. NAS Treatment Plan (Kocherlakota, 2014) Click to enlarge |
The ultimate goal of both pharmacological and non-pharmacological treatments is to reduce suffering and improve the infant's growth and entrance into their new life. It is essential to understand that each case is highly variable based on the addicting drug, the length and severity of addiction, the symptoms shown by the infant, and more. Advances are frequently followed by set-backs, and successful weaning could take weeks to months. Despite these giant hurdles, hope for recovery is found in the caring arms of nurses and physicians who are dedicated to providing relief from this challenging start to life (Hudak et al, 2012).
References
Hudak, M., Tan, R., The Committee on Drugs, & The Committee on Fetus and Newborn. (2012) Neonatal drug withdrawal. Pediatrics, 129(2), 540-560. doi: 10.1542/peds.2011-3212.
Kocherlakota, P. (2014). Neonatal Abstinence Syndrome. Pediatrics, 134(2), 547-561. doi: 10.1542/peds.2013-3524.
No comments:
Post a Comment